

Dr Anita Nathan Identifies Key Learning Points for Primary Care from a Best-practice Guide to Managing Malnutrition in COPD
| Read This Article to Learn More About: |
|---|
Find key points, COVID-19 considerations, and implementation actions for STPs, ICSs, and clinical pharmacists in general practice at the end of this article |
Chronic obstructive pulmonary disease (COPD) is a progressive lung disease caused by chronic inflammation and damage to the respiratory system. It results in restricted airflow causing breathing difficulties.1 Around one in three inpatients2 and one in five outpatients3 with COPD are at risk of malnutrition. Malnutrition is an imbalance of energy, protein, and other nutrients that causes adverse effects on the body (shape, size, and composition), its functions, and clinical outcomes.4
Malnutrition can develop over several years or be precipitated by an acute exacerbation of COPD. The causes of malnutrition in patients with COPD are varied and include:1
- psychological, social, and environmental factors e.g. depression, social isolation, and poverty
- medication e.g. taste changes and dry mouth secondary to oxygen therapy
- physiological effects of the disease e.g. breathlessness and fatigue that reduce appetite and the ability to eat
- increased nutritional requirements e.g. energy and protein.
Individuals with COPD may have increased nutritional requirements arising from systemic inflammation and the increased effort associated with breathing. As their disease progresses, people with COPD may experience infective exacerbations with consequential reduction in their body mass index (BMI) and skeletal mass and strength, in the form of sarcopenia or cachexia.5,6
For people with COPD who are malnourished and underweight, the consequences are significant and can further impair nutritional intake7 and lead to reduced muscle strength and respiratory muscle function, more hospital admissions, longer hospital stays, and higher mortality rates.1 The annual health and social care costs of managing patients with malnutrition are more than three times greater than those of managing non-malnourished patients.1 Therefore, it is essential for both the patient and the healthcare system that malnutrition is proactively and effectively managed in people with COPD.
Managing malnutrition in COPD1 is a best-practice guide launched in 2016. Developed by a multi-professional expert panel, it collates clinical evidence, clinical experience, and best practice to support primary care professionals incorporate malnutrition screening and management in COPD care pathways. The guide is endorsed by 10 professional and patient associations and includes an endorsement statement from NICE. In January 2020, a second edition of the guide was published to incorporate:
- recent NICE guidance (NICE Guideline [NG] 115, Chronic obstructive pulmonary disease in over 16s: diagnosis and management)8
- the Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy9
- updates on energy and protein requirements for people with COPD10–12
- revised advice on nutritional intervention alongside pulmonary rehabilitation programmes that have been found to improve patient outcomes.8,13–16
The Managing malnutrition in COPD guide includes information on screening for malnutrition as well as on management and is supported by three patient information leaflets that are free to download:
- Eating well for your lungs for those at low risk of malnutrition (www.malnutritionpathway.co.uk/library/green.pdf)
- Improving your nutrition in COPD for those at medium risk of malnutrition (www.malnutritionpathway.co.uk/library/yellow.pdf)
- Nutrition support in COPD for those at high risk of malnutrition (www.malnutritionpathway.co.uk/library/red.pdf)
This article highlights the key learning points for primary care from the Managing malnutrition in COPD guide.
1. Screen for Malnutrition Routinely
NICE Guideline 115 recommends routine nutritional risk screening for all individuals with COPD across all settings using a validated screening tool. It also recommends that BMI is calculated in all patients with particular attention to unintentional weight loss in older people.8
The Malnutrition Universal Screening Tool (MUST)17 is a validated, simple, and widely used five-step screening tool that combines assessment of BMI, recent unplanned weight loss, and presence of acute illness to generate a malnutrition risk score (see Figure 1). It can be embedded in existing COPD care pathways with regular recording of weight. The MUST is integrated in Managing malnutrition in COPD,1 which outlines the appropriate management options for people who are at low, medium, and high risk of malnutrition and includes information on monitoring intervals.

[A] The ‘Malnutrition Universal Screening Tool’ (‘MUST’) is reproduced here with the kind permission of BAPEN (British Association for Parenteral and Enteral Nutrition). For more information and supporting materials see www.bapen.org.uk/musttoolkit.html
[B] Treat, unless detrimental or no benefit is expected from nutritional support e.g. imminent death
MUST=Malnutrition Universal Screening Tool; BMI=body mass index; COPD=chronic obstructive pulmonary disease; ONS=oral nutritional supplements
Elia M, editor. The ‘MUST’ report. Nutritional screening for adults: a multidisciplinary responsibility. Redditch: BAPEN, 2003. Available at: www.bapen.org.uk/pdfs/must/must-report.pdf
Adapted from: Anderson L, Banner J, Bostock B et al. Managing malnutrition in COPD. 2nd ed. 2020. Available at: www.malnutritionpathway.co.uk/copd
2. Manage Malnutrition According to Risk
People with COPD who are at low risk of malnutrition should follow general healthy eating advice. The patient information leaflet Eating well for your lungs (www.malnutritionpathway.co.uk/library/green.pdf) provides information on healthy eating along with tips on coping with common symptoms like dry mouth and taste changes. These patients should be rescreened annually or if there is clinical concern.
Obesity, malnutrition, and COPD can coexist. Therefore, when offering dietary advice to overweight or obese patients with COPD, consider the preservation of muscle mass with enough protein.1 Further definitive randomised controlled trials are needed to formulate guidance for the management of obesity in COPD.
People at medium risk of malnutrition should be given dietary advice including information on food fortification. The leaflet Improving your nutrition in COPD (www.malnutritionpathway.co.uk/library/yellow.pdf) contains information and advice. Progress should be reviewed every 1–3 months.
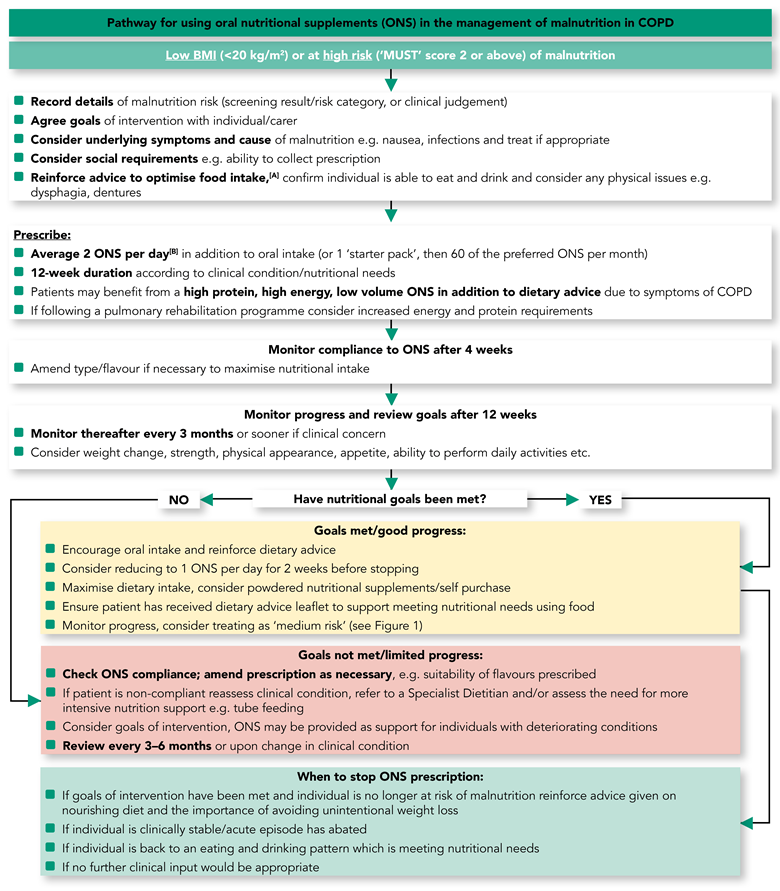
Based on the evidence available, people at high risk of malnutrition should be given dietary advice as above, and prescribed two oral nutritional supplements (ONS) per day for up to 12 weeks or according to clinical need.1 In addition, NICE recommends that patients with COPD and a BMI less than 20 kg/m2 should be prescribed ONS.8
Figure 2 outlines the pathway for using ONS in the management of COPD, including goal setting, reviewing timeframes, what to do if a patient has not met their nutritional goals, and when to stop an ONS prescription. Compliance with ONS should be monitored after 4 weeks and progress and goals reviewed every 4 weeks thereafter or more often if there is clinical concern. The leaflet Nutrition support in COPD (www.malnutritionpathway.co.uk/library/red.pdf) provides tips on how people can best incorporate ONS in their diet.
[A] Your guide to making the most of your food is available from www.malnutritionpathway.co.uk
[B] Some individuals may require more than 3 ONS per day—seek dietetic advice
ONS=oral nutritional supplements; COPD=chronic obstructive pulmonary disease; BMI=body mass index; MUST=Malnutrition Universal Screening Tool
Adapted from: Anderson L, Banner J, Bostock B et al. Managing malnutrition in COPD. 2nd ed. 2020. Available at: www.malnutritionpathway.co.uk/copd
3. Ensure Nutritional Support is Acceptable and Effective
NICE Guideline 115 recommends that nutritional interventions should be incorporated as part of exercise programmes as this has been found to improve outcomes.8 Regular monitoring is key to effective management of malnutrition in COPD. At each appointment, the acceptability and practicality of nutritional support should be reviewed to ensure the patient is adhering to both dietary advice and ONS, if prescribed. Barriers such as lifelong perceptions about healthy eating, breathlessness, gas trapping, early satiety, reduced mobility, and access to food may cause difficulty in applying dietary advice. The importance of good nutrition to help maintain lung health, overcome infection, and/or improve physical ability to carry out activities of daily living should be discussed with the patient or their carer to support behaviour change.
Clinical evidence illustrates that ONS are a clinically and cost-effective method of nutritional support for patients with COPD at high risk of malnutrition and are associated with clinical benefits including significant improvements in functional outcomes, respiratory muscle strength, exercise performance, and quality of life.1 Muscle protein is directly affected by protein intake in the diet and muscle oxidative metabolism may be stimulated nutritionally;1,18 therefore, high-protein (greater than or equal to 20% of energy from protein) and high-energy (greater than or equal to 2 kcal/ml) ONS may be particularly beneficial to patients with COPD due to their increased nutritional requirements, particularly during pulmonary rehabilitation or acute exacerbations.1 Low ONS volumes (125 ml) are associated with better compliance19 than standard volumes (200–237 ml) and may be more suitable for patients with COPD. Other factors should also be considered when assessing the most clinically appropriate ONS, including the patient’s physical ability to prepare a powdered ONS and any other patient preferences.
4. Refer for Dietetic Input
Dietetic referrals should be incorporated in local pathways of care. Access to dietitians will vary but referral should be considered in people with COPD at high risk of malnutrition who:
- struggle to adopt dietary advice
- have multiple morbidities for which dietary advice is conflicting e.g. diabetes and COPD
- have poor compliance to an ONS prescription
- have continued deterioration in nutritional status or
- fail to respond to the nutritional intervention within 1–3 months.
If there is limited access or long waiting times for dietetic expertise in your area, consider discussing your patient case remotely with a dietitian. It would also be useful to involve your local dietetic department in planning and undertaking potential audits assessing the impact of a nutritional intervention on outcomes in patients with COPD.20,21
Summary
Malnutrition is an important consideration in people with COPD and best practice community guidance is available to support the nutritional care of patients at risk of or experiencing disease-related malnutrition in primary care. Optimising nutritional interventions has been demonstrated to lead to improved clinical and cost-effective outcomes.
Dr Anita Nathan
GP, London
Member of the expert panel for Managing malnutrition in COPD
Member of the GPs Interested in Nutrition Group (an RCGP specialist group)
| Key Points |
|---|
COPD=chronic obstructive pulmonary disease; MUST=Malnutrition Universal Screening Tool; ONS=oral nutritional supplements |
| COVID-19 Considerations |
|---|
|
| Implementation Actions for STPs and ICSs |
|---|
Written by Dr David Jenner, GP, Cullompton, Devon The following implementation actions are designed to support STPs and ICSs with the challenges involved with implementing new guidance at a system level. Our aim is to help you consider how to deliver improvements to healthcare within the available resources.
STP=sustainability and transformation partnership; ICS=integrated care system; PCNs=primary care networks; COPD=chronic obstructive pulmonary disease |
| Implementation Actions for Clinical Pharmacists in General Practice |
|---|
Written by Gupinder Syan, Training and Clinical Outcomes Manager, Soar Beyond Ltd The following recommendation actions are designed to support clinical pharmacists and other primary care healthcare professionals (HCPs) in general practice with implementing the guidance at a practice level.
For more online training, please visit the i2i website join up as a free member to access a 3-part series on managing malnutrition in primary care www.i2ipharmacists.co.uk/members/therapy-areas/?therapy=frailty-in-older-people&insight COPD=chronic obstructive pulmonary disease; MUST= Malnutrition Universal Screening Tool; ONS=oral nutritional supplements; BMI=body mass index; HCP=healthcare practitioner |