

Dr David Watson and Dr Sandeep Sharma Provide an Overview of the Recommendations from the Latest SIGN Guidance on Managing Migraine
| Read This Article to Learn More About: |
|---|
Find key points and implementation actions for STPs and ICSs at the end of this article |
Migraine is the most common severe form of primary headache (a headache that is not associated with an underlying pathology), with a global prevalence of around one in seven people.1 Data from the Landmark study revealed that, of patients attending general practice with episodic disabling headache, 94% had migraine.2 In the age group 15–49 years, migraine is the top cause of years lived with disability.3
Need for a Guideline
In 2008, SIGN published its first guideline on headache: SIGN 107 on Diagnosis and management of headache in adults, which included a section dedicated to migraine.4 Since 2008, chronic migraine has been redefined, new evidence on acute and preventative therapies has become available (botulinum toxin A is now licensed to treat chronic migraine),5 and there is an overall greater understanding about the pathophysiology of migraine. Medication overuse headache (MOH) has become better recognised, and guidance on its management is necessary.
Despite a plethora of guidelines available, evidence suggests that migraine is still under-diagnosed and poorly managed. A cross-sectional study of 10 European countries showed that, in most, fewer than 10% of patients with frequent migraine were receiving adequate acute therapy and even fewer received preventer therapy, despite being eligible.6 It is likely that the situation is similar in the UK.7
In February 2018, SIGN published SIGN 155 on Pharmacological management of migraine,8 which supersedes the recommendations on migraine in SIGN 107. The 2018 guideline focuses on treatment for adults with acute migraine and preventative treatment for adults with episodic migraine, chronic migraine, or MOH, with the aim of improving quality of care and patient outcomes.
Diagnosis of Migraine
Accurate diagnosis of migraine is the key to successful treatment. Diagnosis should be made using the International Classification of Headache Disorders diagnostic criteria (see: ichd-3.org/classification-outline). Practitioners should refer to the definitions of migraine without aura, chronic migraine, and medication overuse headache. Note that in reality, patients may not always meet all the criteria. In a busy general practice, headache diaries can be helpful to quantify the number of headache days and other migraine symptoms. It is useful to ask the patient what they would like to do when they have a headache; most patients with migraine prefer to keep their head still when the pain is bad but may not necessarily lie down. Some patients may have to stop activities. Patients with tension headache, which is featureless, tend not to be disabled so are less likely to consult a doctor. Patients with cluster headache are very disabled by pain and agitation but the headache is short-lived, usually lasting about 1–2 hours (migraine tends to last at least 4 hours if untreated). Headache with a sinus source is rare and most frontal headache will be migraine. It is important to be aware that only about one-third of migraine patients get aura,9 40% will get bilateral pain,9 and at least 50% will get neck pain.10 Dizziness is also common, with a lifetime prevalence of 18%.11
Treatment
Medication for migraine is classified as either acute or preventative.
Acute treatment is used either to abort an attack of migraine or to significantly reduce the severity of the headache and other symptoms. Preventative treatment is taken continuously to reduce the frequency and severity of migraine attacks. Often a combination of acute and preventative treatment is needed.
For treatment to be effective, it is crucial that the correct diagnosis has been made.
Please note that not all of the treatments discussed in this article currently (May 2018) have UK marketing authorisation for the indications mentioned. The prescriber should follow relevant professional guidance, taking full responsibility for all clinical decisions. Informed consent should be obtained and documented. See the General Medical Council’s guidance on Good practice in prescribing and managing medicines and devices12 for further information.
Refer to SIGN 155 for information about treatments in pregnancy.
Acute Treatment
Acute treatment works best if it is administered as early as possible in the migraine attack, before central sensitisation of the brain develops.8,13 Once this ‘brain wind-up’ occurs, treatments tend to be less effective. For this reason, patients who wake with a migraine often find it difficult to treat.
SIGN 155 recommends using either simple analgesics (aspirin 900 mg or ibuprofen 400–600 mg) or triptans (sumatriptan 50–100 mg) as first-line treatment. If sumatriptan is prescribed and the response is inadequate, try sequencing through different triptans. Practitioners may also consider prescribing a combination of sumatriptan (50–85 mg) and naproxen (500 mg). Specific points on using triptans are listed in Box 1. Antiemetics (metoclopramide 10 mg or prochloroperazine 10 mg) are recommended for patients who experience symptoms of nausea or vomiting. Both metoclopramide and prochloroperazine have direct analgesic effects and so can be helpful even in patients who have little gastric upset, in combination with simple analgesics or a triptan.8
| Box 1: How to Use Triptans8 |
|---|
Triptans only work once the headache starts
|
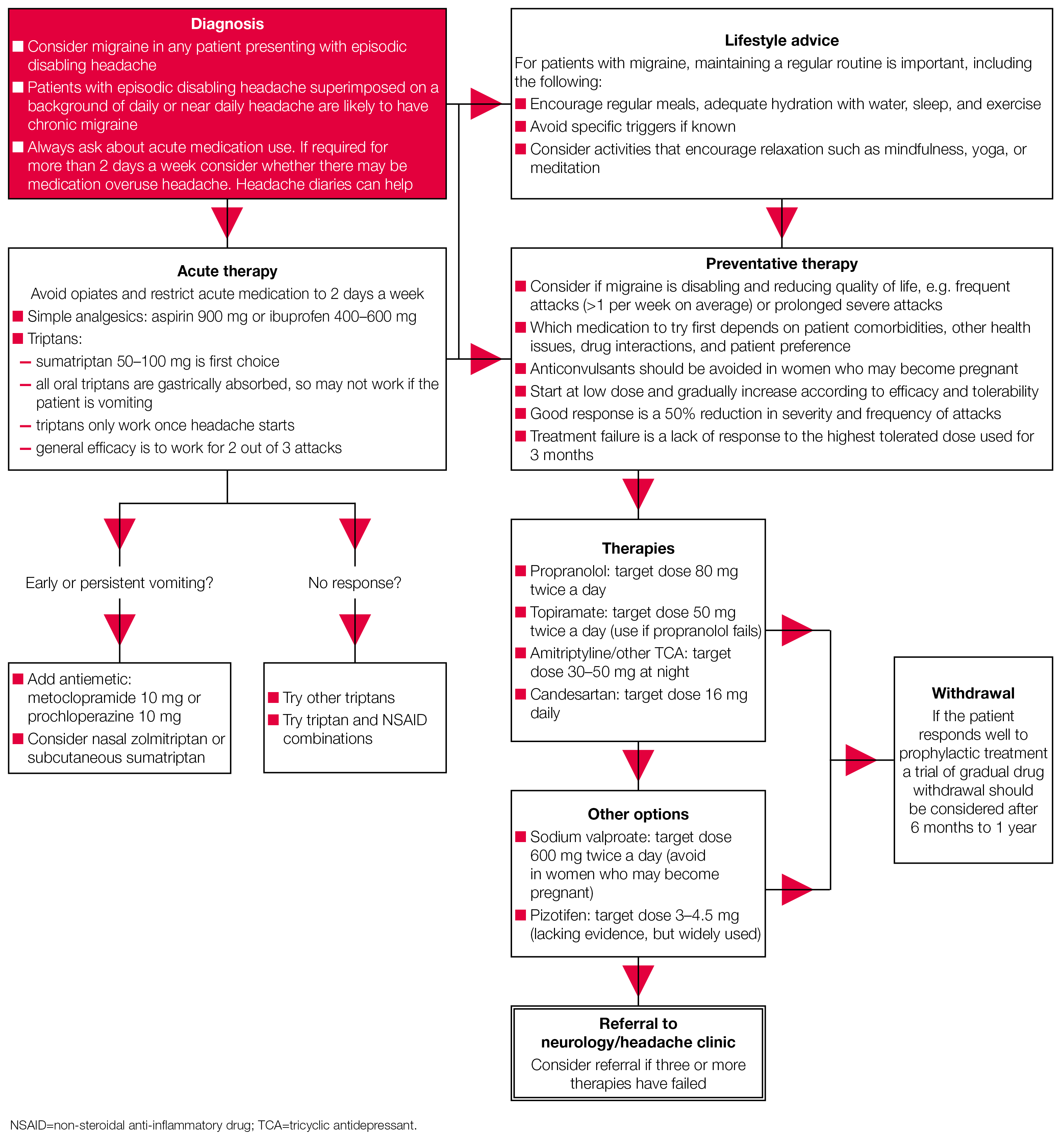
Table 1 lists the number needed to treat (NNT) to achieve an outcome of pain free at 2 hours for several acute migraine therapies—note that the list of therapies is not exhaustive. It shows that sumatriptan (administered as a subcutaneous injection) is the most effective treatment, and paracetamol is the least effective. Acute treatment will not always work for every migraine, and patients should be offered appropriate rescue medication for this situation. For example, subcutaneous sumatriptan may be appropriate in some patients who do not respond to an oral or nasal triptan. The risk of MOH should be discussed with every patient started on acute treatment.8 The algorithm for pharmacological management of migraine, shown in Figure 1, outlines good practice in acute treatment.
There are a number of devices that are marketed as helpful in treating migraine symptoms. The SIGN guideline development group found no robust evidence to make any recommendations for any of them.8
Table 1: Calculated Numbers Needed to Treat for Acute Migraine Therapies for an Outcome of Pain Free at 2 Hours in Patients with Moderate to Severe Pain, Compared with Placebo8
| Therapy | NNT |
|---|---|
| Simple analgesics | |
| Aspirin 900 mg or 1000 mg | 8.1 |
| Diclofenac potassium 50 mg | 8.9 |
| Ibuprofen 400 mg | 7.2 |
| Ibuprofen 200 mg | 9.7 |
| Naproxen 500 mg or 825 mg | 11 |
| Paracetamol 1000 mg | 12 |
| Oral triptans | |
| Sumatriptan 50 mg | 6.1 |
| Sumatriptan 100 mg | 4.7 |
| Zolmitriptan 5 mg | 4.8 |
| Zolmitriptan 2.5 mg | 5.0 |
| Nasal sprays | |
| Sumatriptan 20 mg | 4.7 |
| Zolmitriptan 5 mg | 3.0 |
| Subcutaneous injection | |
| Sumatriptan 6 mg | 2.3 |
| Combination therapy | |
| Sumatriptan 50–85 mg and naproxen 500 mg | 4.9 |
| NNT=number needed to treat | |
| Scottish Intercollegiate Guidelines Network (SIGN). Pharmacological management of migraine. SIGN 155. SIGN, 2018. Available at: sign.ac.uk/sign-155-migraine.html | |
Source: Scottish Intercollegiate Guidelines Network (SIGN). Pharmacological management of migraine. SIGN 155. SIGN, 2018. Available at: sign.ac.uk/sign-155-migraine.html
Preventative Treatment
Regular, preventative medication should be considered for patients with chronic or episodic migraine. The decision to start treatment should be guided by the impact of migraine on the patient’s quality of life, rather than the absolute number of migraines experienced per month. Even modest improvements in the frequency or severity of migraine headaches can provide considerable benefits to an individual; within trials, a reduction in migraine headache severity and/or frequency of 30–50% is regarded as a successful outcome. Guidance on starting and stopping preventer medication is provided in Box 2.
| Box 2. Guidance on Starting and Stopping Migraine Preventer Therapy8 |
|---|
|
SIGN 155 recommends propranolol 80–160 mg daily or topiramate 50–100 mg daily as these medicines have the best evidence base. All medications should be reviewed if pregnancy is planned—topiramate is contraindicated in pregnancy due to the risks to the unborn baby.
If propranolol or topiramate are not tolerated or are contraindicated, other medications that can be considered are:8
- amitriptyline 25–150 mg at night (or a less sedating tricyclic antidepressant if amitriptyline is not tolerated)
- candesartan 16 mg daily—it has a good side-effect profile with no potential cognitive effects; however, the evidence base is small and further trials are unlikely to be conducted
- sodium valproate 400–1500 mg daily—prescribers should be aware that sodium valproate is associated with an increased risk of foetal malformations and poorer cognitive outcomes in children exposed to valproate in utero. Prescribers need to be aware of the current MHRA advice on safe prescribing.14
If treatment with three or more oral prophylactic therapies has failed, botulinum toxin A is recommended for patients with chronic migraine (not episodic migraine), where medication overuse has been addressed.8
It is worth noting that SIGN advises against using gabapentin for the prophylactic treatment of migraine.8
There was insufficient evidence to support a recommendation for:8
- pizotifen
- pregabalin
- SSRIs and serotonin norepinephrine reuptake inhibitors (SNRIs)
- angiotensing-converting enzyme inhibitors.
The only calcium channel blocker with supporting evidence in treating migraine is flunarizine, which is not licensed in the UK. Provision of flunarizine is normally via hospital prescription by a specialist headache service.8
A suggested prophylaxis treatment pathway is included in the algorithm in Figure 1.
Medication Overuse Headache
Medication overuse headache (MOH) is where frequent use of acute treatments for migraine increases headache intensity and frequency. Most MOH is a complication of migraine.8 The following are accepted causes of MOH:15
- use of triptans, ergots, combination analgesics and/or opioids on 10 or more days per month
- use of simple analgesics on 15 or more days per month.
Risk factors for the development of MOH include frequent headache, another painful condition requiring analgesia, and psychiatric co-morbidity. Importantly, not all patients overusing acute treatments have MOH, and some just have poorly treated migraine. Withdrawing the overused medication can reduce headache frequency and intensity, although initially withdrawal is often associated with transient worsening of headache. There is no strong evidence on what the best withdrawal strategy is; Box 3 summarises the options available. The SIGN guidelines states that prednisolone should not be used in the routine management of MOH. Although naproxen is often used in clinical practice as a transitional treatment there is no evidence for its use in patients with MOH. It is important to inform patients about MOH before starting acute treatment.8
| Box 3: Medication Overuse Withdrawal Strategies8 |
|---|
The choice of strategy to address medication overuse should be tailored to the individual patient and may be influenced by co-morbidities. Strategies include:
Consider withdrawing strong opioids gradually. |
Barriers to Implementation
SIGN 155 provides clear advice on the management of migraine. An accurate diagnosis is essential to manage migraine effectively. Patients are often misdiagnosed as having ‘tension headache’ or ‘sinus headache’ or no diagnosis is given.7,16 General practitioners should be aware of the Landmark study2 mentioned at the outset of this article, which reported that of patients attending GPs with episodic disabling headache, 94% had migraine.2 Barriers to doctors making a diagnosis include lack of formal headache training, lack of confidence in making a diagnosis, and time pressures.7
At the secondary care level, there are only a few neurologists with a headache interest and while numbers of GPwSI in headache are growing (albeit slowly) there are many parts of the UK that do not have a headache service.7 This makes access to therapies such as flunarizine and botulinum toxin difficult for patients.
Conclusion
SIGN 155 provides an evidence-based update on the medical management of migraine. Probably the most useful section for GPs and nurse practitioners is the migraine treatment pathway found in Annex 3 of the guideline, and reproduced in this article (see Figure 1). In summary, if a patient attends general practice with disabling episodic headache they most likely have migraine and should be provided with effective acute therapy and prophylaxis depending on the extent of disability and co-morbidities. See Box 4 for a list of useful sources of information for patients and healthcare professionals.
| Box 4: Useful Sources of Information |
|---|
|
Dr David PB Watson
GP partner, Hamilton Medical Group, Aberdeen
GPwSI headache, Department of Neurology, Aberdeen Royal Infirmary
Member of the guideline development group for SIGN 155
Dr Sandeep Sharma
GP, Bonnybridge
Member of the guideline development group for SIGN 155
| Key Points |
|---|
|
| Implementation Actions for STPs and ICSs |
|---|
Written by Dr David Jenner, GP, Cullompton, Devon The following implementation actions are designed to support STPs and ICSs with the challenges involved with implementing new guidance at a system level. Our aim is to help you consider how to deliver improvements to healthcare within the available resources.
STP=sustainability and transformation partnership; ICS=integrated care system |