

Dr Sadaf Haque Offers 10 Top Tips for Primary Care on the Identification and Management of Mental Health Problems in Adults with Cancer
| Read This Article to Learn More About: |
|---|
|
Anxiety and depression are more prevalent in patients treated for cancer than in the general population.1 Significant psychological morbidity can be associated with receiving a cancer diagnosis (which can vary between cancer sites2), or be precipitated and exacerbated by consequences of treatments. Pre-existing severe mental health problems may also increase cancer risk because chaotic and risky behaviours alongside poorer lifestyle choices can make it more difficult to safety-net and for people to adhere to follow up. Stress can also result in biological changes that increase cancer risk.3
However, the psychological impact of cancer may not always be negative and many people will not experience problems with depression and anxiety. Experiencing temporary distress related to a cancer diagnosis may lead to positive psychological changes in the long term, whereby individuals feel a greater appreciation of life and are able to re-evaluate their priorities.4
The tips in this article focus on how primary care can support patients with cancer and mental health problems, including considerations for this group during the COVID-19 pandemic.
1. Recognise the Psychological Effects of Cancer and its Treatment
Psychological difficulties commonly associated with cancer treatment, post-treatment recovery, and adjustment include:5
- anxiety and depression (from mild to severe)
- phobias and panic attacks
- problems with interpersonal relationships, which may also extend to healthcare professionals
- psychosexual and body image difficulties
- deliberate self-harm
- psychotic illness
- cognitive impairment
- post-traumatic stress disorder.
Cancer treatments may directly or indirectly affect the patient’s mental health, for example:1,6
- immunotherapy and chemotherapy may induce depression through biological mechanisms
- medications used to treat chemotherapy-induced nausea can reduce dopaminergic transmission, which is implicated in the development of depressive symptoms
- steroids in cancer treatment can induce depression
- androgen deprivation therapy in the treatment of prostate cancer is also associated with increased risk of depression
- prostate cancer treatment may be associated with incontinence and sexual dysfunction.
There are certain points in the patient’s cancer journey where it is important to pay particular attention to their mental health, for example, when their active treatment ends or when there is new information about their prognosis.
2. Use Open Questions to Promote a Discussion about Psychological Wellbeing
Elicit concerns as patients may not volunteer them: many mental health problems in patients with cancer are missed because patients don’t divulge the information and health professionals don’t invite it.7 Some useful openers include:
- ‘How are you coping?’7
- ‘Do you have some other concerns you would like to discuss today?’. Use this rather than, ‘Do you have any other concerns…?’ (‘Some’ elicits significantly more concerns than ‘any’)8
- ‘What are you worried will happen?’
- ‘What else would you like to know?’ (50–75% of patients who want more information don’t ask for it in medical consultations. Information facilitates adjustment, especially in the early phases of treatment if patients experience excessive fear).9
Be mindful of how your language may shape what kind of problems a person feels it is acceptable or legitimate to experience and discuss; for example, avoid language around ‘being a fighter’. Acknowledge emotional distress and anxiety in a non-judgemental way and discuss the forms of support available.
Assessing for depression is not straightforward in people with cancer because:6
- as in the context of bereavement, sadness is normal and an adaptive reaction
- the physical impacts of affective disorders (for example, on appetite, sleep, weight) will be confounded by the effects of cancer/cancer treatment.
Ask about psychological rather than physical features to assess depression, which may include:
- inability to experience pleasure
- feelings of guilt
- worthlessness
- withdrawal
- blaming self for feeling a burden
- pervasive hopelessness.
Try to ascertain what has contributed to, exacerbated, or is maintaining depression as there might be scope to offer support with some factors directly.
Helping patients focus on what they can control is vital to reduce the likelihood of anxiety and depression. It can be helpful to normalise the patient’s reactions and feelings and also to outline a treatment ‘road map’ (although the detail will need to be provided by the hospital service the patient is accessing for their cancer care). Planning in follow-up appointments can help patients feel less abandoned.
Discuss with patients how diet, exercise, monitoring their energy levels, and staying engaged with normal roles and responsibilities as far as possible are all important for mental health. Such self-management could help prevent distress becoming clinical depression or anxiety.
If you are considering offering medication to help with affective disorders, check there is no potential side-effect or interaction that may affect the efficacy of cancer treatments.
3. Understand the Patient’s Psychological Health
The very experience of being diagnosed with cancer, particularly if delayed, can be a significant source of distress, anxiety, and feelings of loss of control and uncertainty around survival and death; especially with a cancer stage that has a poor prognosis. The levels of intrusive thoughts during the early phases of cancer have been found to predict depression and anxiety 6 months later.9 Depression can include feelings of hopelessness, with patients feeling guilt and blaming themselves for poorer lifestyle choices, for example, lifelong smoking and a lung cancer diagnosis.1
Uncertainty, dependence, and loss of control are three of the hardest factors patients report experiencing. Other common emotions are: anger, fear, shame, anticipatory anxiety, reduced confidence, hopelessness, body image concerns, existential/spiritual concerns.10
Adjustment is not a one-off event, it is a process so be wary of patients wanting to be seen as ‘coping’— it can be helpful to debunk the belief that the open expression of feelings means they are ‘not coping’.
Living with and beyond cancer is an experience that disrupts implicit assumptions about life, and forces people to reconstruct their perspectives on self and future. The Adversity, restoration, and compatability (ARC) framework may help people to make sense of their cancer experience (see Figure 1).5,11
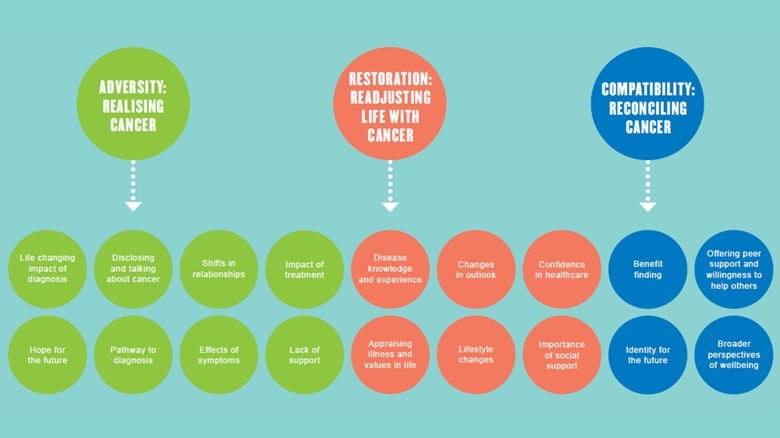
The ARC framework: adversity (realising cancer), Restoration (readjusting life with cancer), and compatibility (reconciling cancer). The themes are interlinked because the experience of living with and beyond cancer is non‐linear. People affected by cancer can move backwards and forwards between themes as well as straddle across themes
Le Boutillier C, Archer S, Barry C et al. Conceptual framework for living with and beyond cancer: a systematic review and narrative synthesis (supplemental data). Psycho-Oncology 2019; 28: 948–959.
Reproduced under the terms of the CC-BY 4.0 licence.
The long-term effects (those that begin during treatment and continue afterwards) and late effects of cancer treatment (those that begin after treatment is completed), such as secondary cancers, infertility, chronic pain, and insomnia, are also likely to affect the mental wellbeing of cancer survivors.
GPs will be receiving patients’ cancer treatment summaries, which are informed by individuals’ holistic needs assessments (HNAs) and subsequent care plans, and include details of the potential long-term and late side-effects of treatment. Cancer support workers are now supporting cancer nurse specialists to continue person-centred care at the point of diagnosis, with HNA/care plans repeated at key points, such as at the end of a treatment phase or when the patient requests a revision. The Macmillan Cancer Support/Royal College of General Practitioners Consequences of cancer toolkit can help primary care clinicians understand what they can do to help people experiencing adverse consequences of cancer but also recognise when and how to involve secondary care.12
4. Signpost Sources of Support
Clinicians should support patients psychologically from diagnosis, while also appreciating that their needs and symptoms may also change over time. It is important to signpost available support options (including peer support) early on in a patient’s cancer pathway (see Box 1). To minimise the psychological impact of cancer, ensure that the patient knows who to ask to clarify the specifics of their pathway.7 Only around one-third of patients with cancer and related psychological distress may be willing to be referred for support13 but patients value having the option to talk about their emotions, with whom and when they choose to.
Social support is the single most important resource for helping with ‘coping’, it can really be a psychological ‘shock absorber’, buffering people from the stressful effects of cancer.14 Be cautious about assuming patients have sufficient support, they often ‘don’t want to be a burden’ or they want to protect family/friends from their concerns. Ask questions to assess their situation, such as:
- ‘What’s helped you cope in the past?’ ‘How have you coped with adversity before?’
- ‘Who are the people who are significant to you?’ ‘What do they know?’
- ‘What’s made you decide not to talk about it?’
| Box 1: Sources of Support for Patients Living With and Beyond Cancer |
|---|
|
5. Offer Training for Practice Nurse Colleagues
The benefits of devolving cancer care reviews to appropriately trained practice nurses are being increasingly realised: patient experience is improved, the patient has a ‘point of contact’ other than the GP, and there is a subsequent shift in GP capacity to focus on other priority areas.15,16
It is therefore important to train practice nurses in conducting effective cancer care reviews using a template, such as that based on the Macmillan Cancer Review.17 Macmillan Cancer Support has produced a guide with the required information and knowledge needed to run a Macmillan Cancer Course for Practice Nurses.18
6. Support the Patient’s Carers, and Patients Who Are Carers
Being a carer for someone with a health condition or disability can have a significant impact on the carer’s own mental health and wellbeing. Supporting the mental health and wellbeing of carers should be a consistent part of a patient’s care plan. The needs of carers have been shown to be rarely considered (therefore rarely met): 67% of carers experienced anxiety and 42% experienced depression, and over three-quarters did not receive any support.19
Ask about reactions of family members (especially children) who might need support and signpost to appropriate third-sector partners such as Maggie’s (www.maggies.org) or Winston’s Wish (www.winstonswish.org), who are often well placed to support families. Also ensure that carers are signposted to partners such as Carers UK (www.carersuk.org).
7. Identify People at Increased Risk of Developing Mental Health Problems
It is important to identify people who are at high risk of developing mental health problems or worsening mental health following their cancer diagnosis and within their own personal, cultural, and familial contexts.20 Existing mental health issues are also a major risk factor for physical ill health, contributed to by socioeconomic determinants and making poorer lifestyle choices—for example, by smoking, which in turn increases cancer risk.7,21 Some of these risk factors are discussed in more detail in Box 2.
A biopsychosocial model of health can also help in identifying those at risk of developing more serious mental health problems (see Figure 2).20
| Box 2: Risk Factors for Mental Health Problems in Patients With Cancer |
|---|
Age Although cancer incidence increases with age, depression is more likely among younger patients and also among those more socially disadvantaged.22 Elderly cancer patients are less likely to volunteer emotional symptoms and are thus particularly vulnerable to being under-diagnosed and under-treated for depressive symptoms.23 Patients and clinicians may be confounded by attributing such symptoms to normal ageing and co-morbidity. Cancer Site Major depression affects more people with lung, gynaecological, breast, colorectal, and genitourinary cancers.22 Contributing factors are complex and variable such as prognosis, pain, body image, and the neuropsychiatric tumour and treatment-related effects.6 People who have accessed mental health services before a cancer diagnosis may experience excess mortality due to certain cancers.3,24 Cancer Survivors Anxiety is more prevalent than depression among cancer survivors (and their spouses), and may be due to poor social support, impaired quality of life, pain, and burden of disease.25 Ethnicity For black and minority ethnic (BAME) communities, a cancer diagnosis may be accompanied by stigma perceived individually or by their community, or there may be a language barrier to open communication.26,27 Gender For lung and colorectal cancer, being female is a risk factor for adverse mental health.22 Learning Disability Mental health problems are more prevalent in people with learning disability than in the general population.28 It is worth keeping this in mind in the context of cancer. Smoking Smoking rates in the UK are three times higher among people with a mental health condition than in the general population. This risk factor may be compounded by patients being less likely to engage with health promotion interventions (such as smoking cessation support), present for timely investigation of concerning symptoms (e.g. haematuria), or to take up screening offers.7 Socioeconomics Health and social care inequalities also impact early diagnosis of cancer and there are equally well documented inequalities in cancer survival.29–31 People affected by socioeconomic factors—for example, unemployment, fewer educational qualifications, lack of social support, or lack of access to timely welfare support (e.g. disability benefits)—may also experience significant financial consequences from their cancer. |
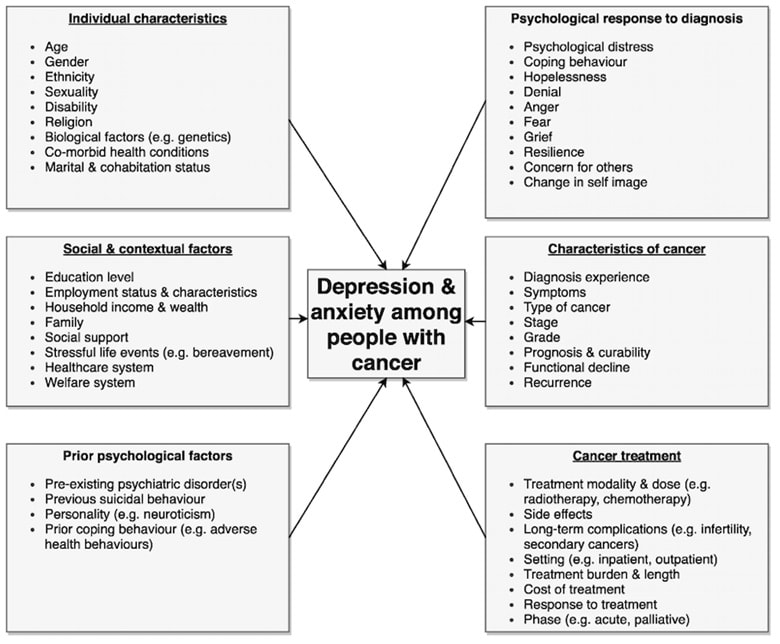
Niedzwiedz C, Knifton L, Robb K et al. Depression and anxiety among people living with and beyond cancer: a growing clinical and research priority. BMC Cancer 2019; 19: 943. Reproduced under the terms of the CC-BY 4.0 licence.
8. Assess Risk of Suicide and Identify Red Flags for Referral
Certain groups of patients are more vulnerable to thoughts of suicide, for example, those with cancer and co-existing severe mental illness.
People with cancer have a 20–55% higher risk of suicide than people without cancer.2,32 Those with poorer prognosis cancers (such as mesothelioma, pancreatic, lung, head and neck, gastric, and pancreatic) have a higher suicide risk, especially within the first 6 months of diagnosis. Other factors associated with suicide risk are hopelessness, demoralisation, lack of control, uncontrolled pain, depression, advanced disease/poor prognosis, previous suicide attempts by either the patient or a family member, exhaustion/fatigue, lack of social support, and substance/alcohol use.33,3
Safety-netting is very important in this at-risk group. Be explicit about advice to return with concerns about mood, worries, or mental health. Patients often need permission to disclose these concerns, especially to doctors. Asking patients about suicidal thoughts does not encourage patients to act on them.
Assess suicidal ideation using graded questions, especially about hopelessness for the future. If the patient has had suicidal thoughts, it can help to explore and potentially address the reasons why, for example:9
- poorly controlled symptoms—review their pain relief and consider other palliative support
- loss of control of their life—look at areas where they still have some control
- depression—consider antidepressants and talking therapies.
9. Know What Psychological Support Services are Available for Referral
For GP referrals for talking therapies, the first access is usually through the local Improving Access to Psychological Therapies (IAPT) service, as for patients without cancer. Although cancer is now coded as a long-term condition in IAPT,5 it has not been a specific area for development as yet in the service which, since April 2018, has been integrated into physical healthcare pathways under guidelines to cover long-term conditions.35
Most acute trusts have cancer psychology services that see patients during and for a period after active treatment. They support patients to access cancer investigations, treatment, and post-treatment care and offer highly specialist clinical care for inpatients during medical admission and for outpatients, as well as input for families and carers. Patients should usually speak to their clinical nurse specialist or a doctor at the hospital to access these services.
Clinical Nurse Specialists (and some allied health professionals) should also have access to psychological skills training and supervision to fulfil peer review requirements, so are a good first port of call for patients with cancer presenting with psychological distress or mental health problems.
The main focus of interventions remains to treat the patient’s anxiety or depression in the context of their long-term condition.35 Patients may prefer to be seen in an acute setting, alongside their medical treatment. They can also perceive the referral to be less stigmatising to be seen in the hospital, rather than being referred to a mental health service elsewhere.
Primary and community teams should also be able to access expertise from psycho-oncology teams, thus improving patient experience and outcomes for all those affected by cancer as well as their families and carers.5
10. Support People to Re-engage with Health Services During the COVID-19 Era
The COVID-19 pandemic has significantly disrupted cancer care, impacting current patients as well as future patients who are likely to have a delay in diagnosis. The worry about contracting coronavirus and confusion about shielding advice has meant that fewer people are going to their GP with symptoms that might be suggestive of cancer, and some GPs may be reluctant to risk a referral to hospital for investigation.36 COVID-19 has greatly reduced throughput of already challenged services such as endoscopy and cancer surgery; a common feature of emergency national guidelines is balancing COVID-19 risk against the risk of non-engagement with clinical recommendations.
It is important for patients to understand that consultations can be done remotely by telephone or video. Where advised to come into a healthcare setting for tests or treatment, the patient should be reassured that there are measures in place to safeguard both patients and staff, and that personal protective equipment (PPE) is available.
Spreading public awareness messages, such as the NHS England ‘Help us to help you’ drive37 and the Cancer Research UK Coronavirus and cancer video,38 will encourage people to present to their GP if they have worrying symptoms and to feel comfortable with cancer investigations and treatments in an adapted, safe COVID-19 hospital environment.
Summary
Support people to seek medical advice if they are worried about a symptom. Make contact with patients if they are diagnosed with cancer, assess their psychosocial risk with open questions and discuss what support can be offered. Many patients are living with cancer as a long-term condition and may benefit from regular cancer care reviews including robust safety-netting, particularly for those at greater risk of mental health problems associated with their cancer.
Dr Sadaf Haque
GP and Clinical Lead for Cancer, One Gloucestershire ICS (Macmillan GP Facilitator)
Acknowledgement
The author would like to thank Dr Hilly Webb-Peploe, Consultant Clinical Psychologist and Lead for Cancer, Haematology and Palliative Care, Gloucestershire Hospitals NHS Foundation Trust, for her valued input into this article.
| Context |
|---|
Cancer is increasingly considered to be a long-term condition (LTC); based on 2012–2016 data, there has been an increase in people’s chances of survival across different types of cancer.39 For patients diagnosed with cancer in England in 2015, 1-year survival was 72%—over 11 percentage points higher than in 2000.24 Mental illness also represents a considerable and growing burden in the UK40 and 9 out of 10 adults with mental health problems are supported in primary care.41 A UK study published in 2014 found that people with serious mental illness (including schizophrenia and schizoaffective disorder, depression, dementia, and substance use disorders) who were diagnosed with cancer during the time they were under secondary mental health services had significantly worse survival after cancer diagnosis compared with other local people, independent of cancer stage at diagnosis.42 Additionally, one study of 1538 cancer patients with depression and complete patient-reported treatment data showed that 73% were not receiving potentially effective treatment for their major depression.22 Other studies suggest that people with mental illness may be more likely to present late and therefore with more advanced cancer. Patients diagnosed with bladder and colorectal cancer who have had previous psychiatric admissions, for example, have been found to be at particularly increased risk of death from their cancer, with cancer diagnosis and treatment often affecting psychosocial quality of life.3 A report by the Nuffield Trust stated that 15 months after diagnosis, patients diagnosed with cancer have 60% more A&E attendances, 97% more emergency admissions, and 50% more contact with their GPs than a comparable group.43 Strategic Alignment with NHS Long Term Plan AmbitionsCancer and mental health are strategic priorities in the NHS Long Term Plan (LTP),24,41 and both are areas where primary care (working collaboratively as part of a wider health system) can positively affect patient experience. The LTP recognises this and that the best action to continue increasing cancer survival is, by 2028, to diagnose more cancers at the earlier stages of 1 or 2, rather than at stages 3 or 4, which are known to have poorer survival and quality of life outcomes.24 Focusing on a psychologically informed patient care approach at every step of the cancer patient pathway5 is another aspect of delivering the LTP strategic goal so that by 2021 ‘where appropriate, every person diagnosed with cancer should have access to personalised care, including needs assessment, a care plan and health and wellbeing information and support’.24 A more personalised approach to supporting the psychological health of people with cancer is needed. Some people may not want or require support or treatment, others will be able to self-manage, and some may have more complex needs that require more intensive follow up and support. The LTP’s quality of life metric, to track and respond to the long-term impact of cancer, which will also capture whether a person’s psychosocial care needs have been met, is likely to appear on the national cancer dashboard in the near future.5,24 A low-risk stratified pathway for cancer follow up will be suitable for some patients, who can be directed to a health and wellbeing event and empowered to self-manage with support and advice on whom to contact (and how) if they have concerns about their cancer. It is important to recognise and champion joined-up planning and service delivery from the health and social care system perspective, via Sustainability and Transformation Partnerships and (by 2021) Integrated Care Systems.44 Integrating Physical and Mental Health NeedsThe essential components of an integrated approach towards mental and physical healthcare in England are:7
|